


Besides Cass - UK Trends in Gender Medicine
Having banned puberty blockers, UK paediatric gender transition is largely a thing of the past. But what about the wider state of gender medicine? NHS statistics show it is still on the march.


NOTE: I am not from the UK. But I have followed the debate for years now and have done extensive research to familiarize myself with the institutions involved in gender medicine around the world. If I got something wrong, I apologize in advance and am happy to receive any feedback or corrections! Also, typos might pop up ;-)
Summary:
Despite critical wins in the fightback against the institutionalization of gender-identity ideology in medicine and law, trans-related genital surgeries in 2023 in the UK have more than doubled since 2015
Although such surgeries on minors are not legal in the UK, there is still no evidence that genital surgeries improve the well-being of transidentified individuals at any age. Given their irreversibility and the dishonest public framing, there are questions pertaining to medical ethics despite the patients being adults.
Particularly concerning is the dramatic uptick in ‘female-to-male’ genital surgeries increasing from 25 (2022) to 87 in 2023. Also, female patients undergoing surgery are on average much younger than their male counterparts (i.e. 23 years vs. 44 in 2015)
With 5,627 diagnoses in English NHS clinics, gender dysphoria diagnoses reached an all-time high in 2023. Over the last 11 years, there has been a significant decoupling of gender dysphoria being the primary diagnosis or it being part of a diagnosis bundle. In 2023, only 2,000 of 5,627 diagnoses of gender dysphoria were the prime diagnosis suggesting a more complex patient profile. If the “diagnostic overshadowing” of gender dysphoria remains, this implies that more and more mental health issues are not accurately treated
Data on gender medicine is severely flawed as the patient’s gender identity is recorded, not sex. For instance, almost all patients of the surgical procedure “Sexual Transformation from Male to Female” are recorded as female. Moreover, there has been a severe censoring of information by NHS England as unlike with other surgical procedures age and other patient characteristics are no longer published after 2015.
On the various battlegrounds of the gender wars, the UK stands out: After precedent-setting legal wins to protect ‘gender-critical’ belief in employment and the landmark Cass Review largely finishing off paediatric gender transition, the country seems to have a good shot at containing the most harmful impacts of gender-identity ideology.
But what’s the overall situation in Britain’s gender clinics like? How often is gender dysphoria, for which the main ‘treatment’ is still cross-sex hormones and potentially surgery, still diagnosed? And how prevalent are transgender surgeries? Official NHS hospital statistics from England and Scotland between 2000-2023 allow insights.
As expected, genital surgical procedures and diagnoses have steadily risen since data is available and may be somewhat surprising, reaching their highest levels in the financial year of 2023-2024. Particularly troublesome is a sharp spike in so-called ‘female-to-male’ genital surgeries in recent years which involves the ineffective and complication-ridden practice of phalloplasty. Adding to that is that the female patients are often very young, with an average age of 23 in the last year of available data. Moreover, gender dysphoria also for children and adolescents is diagnosed more often than ever before. Certainly, gender clinics are working through the long waiting lists but if the NHS gender services have not undergone substantial de-programming and prescribe cross-sex hormones and surgeries to a much lesser degree than before, the unevidenced practice of medical transition is performed on more people than ever before. On a positive note: It’s much less prevalent than in other countries.
Not to mention the fact that statistics on medical transition practices have been corrupted: ‘Male-to-female’ patients are recorded as female and vice versa. To protect patient confidentiality, age statistics are censored after 2015. Ironically, no other surgical intervention (as intimate and rare as it may be) has been subject to this type of concealment. Breaking statistics is no trivial matter. It always suggests that there is something to hide and, crucially, it limits the full accountability of those in charge.
Medical transition at any age: Always unevidenced, often irreversible
There is no need here to extensively recite the main insights of the Cass Review. In short: there is no credible evidence that puberty blockers alleviate gender-related distress. Given the very serious side effects, prescribing them as the state-of-art treatment for minors is highly unethical.
It is important to note that up to today no such evidence neither exists for the prescription of cross-sex hormones for both adolescents and adults nor for transgender surgeries. Transactivists, allied doctors and large medical associations disagree. But the studies they cite rely on, small samples and simple post-intervention comparisons stating that (self-reported) gender dysphoria symptoms abated significantly when patients (adolescents and adults) started taking cross-sex hormones and underwent surgery. This is taken as proof that medical transition improves the mental health of dysphoric patients. It’s science-y enough to convince empathetic liberals and politicians alike but in truth, it’s a deeply fallacious statement for various reasons.
The first being: We do not know the counterfactual or hypothetical scenario. To judge whether an intervention is effective, you need two groups of patients, ideally very similar but different in one aspect: One group (treatment group) receives the intervention and the other group, similar in age, socioeconomic, and health background, does not constitute the control group. If you detect sizable improvements in objective mental health parameters and sufficiently large sample sizes, medical transition could be deemed an effective medical treatment. Second, the mental health parameters should not be self-reported because treated individuals could always have an incentive to bias results upwards. This would be a massive undertaking and ethically questionable because medical transition involves the unknown health effects from cross-sex hormones, inevitable sterility and possibly drastic side effects from surgeries. This site lists the most important pieces of research claiming benefits to medical transition. I challenge you to find a study that fits high standards of evidence-based medical research. And remember, medical transition is not akin to other medical procedures: Often it involves sterility and unknown health effects and thus should be under the highest scrutiny possible.
In the politicized world of gender medicine, this is hard to achieve because the social framing mainly emphasizes and highlights stories of happy transitions. While the devastating stories of detransitioners gain traction, they rarely penetrate the liberal bubble in which most transition candidates find themselves. At this point, it seems impossible to conduct counterfactual studies and it remains clear that besides individual reports, there is no established evidence that medical transition improves outcomes. This applies to every age group and even if you are an adult-transition libertarian, it remains an unethical procedure to be conducted given the lack of the evidence and its irreversibility. From German hospital records, we know that nowadays it is the cohort of 18-25 year olds who undergo genital surgeries most often.
What is never reported are studies that hint towards potential harms of medical transition including surgeries. A study of trans-identifying individuals in the US from 2003 to 2023 showing up at the emergency room found that those individuals who underwent genital surgeries had a 12.12-fold higher suicide-attempt risk than the general population and still 5 times higher risk than patients who underwent sterilization for other reasons. A study on Californian individuals between 2012-2018 found that suicide risks shot up for individuals undergoing “male-to-female” genital surgery. This does not prove harm but suggests that people are not flourishing and living their best lives having undergone the whole transition process. These operations come with massive side effects: In August 2024, it became public that a 24-year-old trans-identifying female died due to the complications of phalloplasty, and Ritchie Herron’s story of a botched surgery was viewed 1.8 million times on YouTube. As to the effects of cross-sex hormones, it’s puzzling why nobody looks at the most obvious historical precedent in which young women were put on testosterone (or testosterone-derived anabolic steroids). Thousands of sporty girls were drugged with male sex hormones in communist East Germany to increase strength and gain a competitive advantage. It brought home many gold medals, but the health effects are horrifying. Doped athletes (that includes men and women) had a 2.7-fold higher risk of getting (physically) ill compared to the general population and died on average 10-12 years earlier than comparable non-doped counterparts. Tragically, female athletes saw disproportionately many birth defects in their children and as Elaine Miller, a Scottish physiotherapist and gender-critical feminist explains here so succinctly, this can be traced back to the use of testosterone.
While the (adult) pro-medical transition research is very poor, it has to be said that the ethical circumstances and the current environment make unbiased research to prove definitely that it is not beneficial or even harmful immensely difficult to implement. It exceeds my imagination how a controlled trial on all aspects of medical transition could be implemented, so we might never really know what the hypothetical outcome (mental and physical health) would have looked like had a trans-identifying individual not been offered medical transition.1 However, it remains that there is no evidence of the benefits and purporting there is medical negligence and quite possibly part of the unfolding medical scandal. While banning adult transition is also difficult and potentially questionable, the common middle-ground argument of “adults can do what they want” comes with problems, too. It affirms bodily dissociation when you’re just old enough with an ultimate lie at its core: This surgery will turn the patient into the opposite sex. Also, the rationale for paediatric transition was that it makes passing much easier and was a product of more widespread adult transition. That is, if we let adult transition go unchecked there will be always a demand for childhood intervention.
The corruption of statistics: Self-ID and the concealment of data
A particular feature and not a bug of gender medicine statistics is that official statistics are often seriously flawed. For instance, patients’ sex often does not reflect the actual sex but merely what patients say about themselves. The data source used for this article is the NHS Hospital Admitted Patient Care Activity. While few may have indicated their birth sex, many might just have ticked the sex they wish to be. This is not a minor issue because any stratification by sex is not reliable. Sometimes it can be inferred from the statistic itself, for instance, a “female-to-male sexual transformation” surgery is done on a female patient. This could apply to gender dysphoria diagnoses, so any breakdown by sex needs to be somewhat treated with caution.
The next problematic point is a very trans-exceptionalism style concealment of important data in the NHS Hospital Admitted Care Activity. That is, after the financial year of 2015-2016, the age profile is no longer reported. Censoring the data to the public creates a lack of accountability. It was justified as a means of patient data protection. Interestingly this only covers trans-related medical procedures. Even though all patients are by law required to be 18+, it makes a difference whether the average age is continuously declining or whether it’s mostly 50-year-olds who are undergoing these procedures. This is particularly important for the vast increase in phalloplasties in recent years where the last information about age profile reveals a patient mean age of 23 years (see below). Also, for a every trans identifying individual undergoing genital surgery, there is a multiple of individuals ‘only’ taking cross-sex hormones or having other trans-related surgeries (such as mastectomies). Having more information as to age differences between the sexes seeking medical transition could tell us more about what drives people seeking such extreme measures.
Trends in gender dysphoria diagnoses

On a yearly basis, NHS England publishes detailed data about diagnoses according to the ICD-10 catalog. Every diagnosis and procedure is given a distinct code allowing to compare trends across time. When we look at Figure 1, we can see the very common picture of a diagnostic increase of ‘Gender Identity Disorders’ (ICD-10 F64) which contains subcategories for instance transsexualism and gender identity disorder of childhood. It is important to note that also minors were sometimes diagnosed with transsexualism such that gender identity disorder of childhood does not cover the whole array of gender diagnoses of minors. To economize on words, this will be simply called gender dysphoria from now on. We can see the familiar shift of sex ratios with females being diagnosed with gender dysphoria relatively much more common than males with an almost balanced ratio in 2023. What’s probably the most striking is that the number of diagnoses seems to continue increasing reaching its highest level in 2023 with 5,627 diagnoses. The increase in 2022 was much more pronounced for male than for female patients. A word of caution: Diagnoses by private providers such as GenderGP are not included so the overall number is likely higher. Also, this is English data only, the Scottish, Welsh, or Northern Irish data did not allow us to look at gender dysphoria diagnoses.

When we look at minors (ICD-10 F64.2) (Figure 2), we see a very similar picture to the famous referral graph that made its way around the world and motivated many activists and researchers to give this more attention. Figure 2 indicates as to what happened to the children referred. It shows the annual number of minors receiving a gender dysphoria diagnosis and given what we know about the ideological capture of NHS gender services and the lax prescription practice of puberty blockers, it is likely that many of them received some sort of medical intervention. Interestingly, these diagnoses seem to have peaked in 2022 and declined substantially afterward. To what extent this could be the effect of supervising authorities taking a closer look, parents taking their children to private providers or a combination of both is unclear. While puberty blockers are now banned indefinitely, cross-sex hormones are still available at age 16. From an economic point of view, private providers might likely ramp up the prescription of cross-sex hormones if demand for this medication does not severely slow down. Since there is no evidence to suggest the latter, the move towards cross-sex hormones in the NHS and private clinics is something to keep an eye on. TransgenderTrend recently highlighted a court case in which a mother of a trans-identifying child wants to extend consent of both parents to medical treatment outside the NHS beyond 16 years. If she fails, children could decide to access cross-sex hormones without parental consent once they reach the age of 16.
It is not clear what fraction of individuals receiving a gender dysphoria diagnosis are put on puberty blockers, cross-sex hormones, or eventually surgery. But given how deeply gender-identity ideology has captured institutions like the NHS and in the absence of large-scale ideological deprogramming, it is likely that a high share of those receiving a diagnosis will eventually be undergoing any form of medical transition. With gender dysphoria diagnoses reaching their peak in 2023, there is no indication that fewer people undergo this unevidenced treatment.
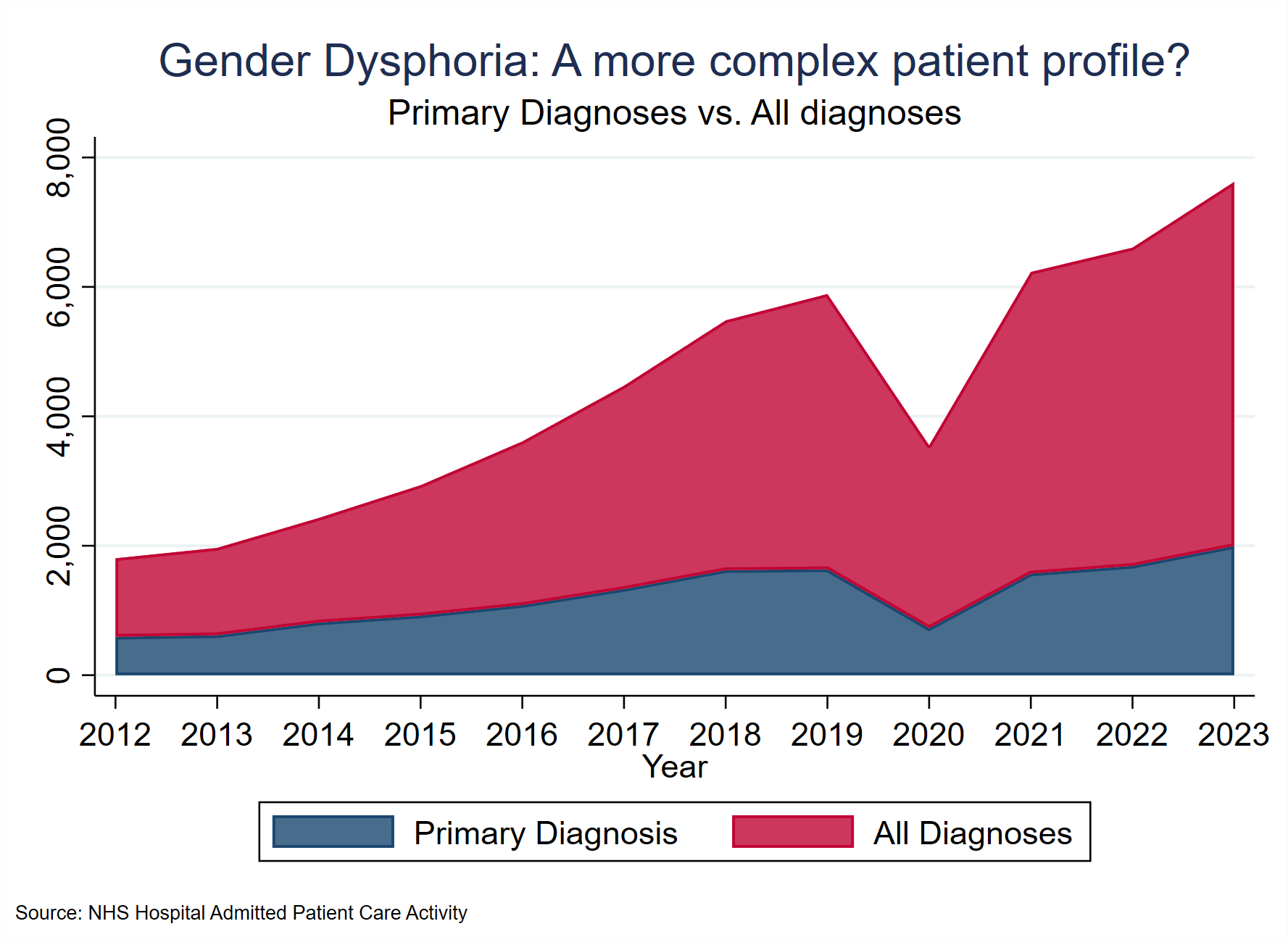
As a final remark on trends in gender dysphoria diagnoses, Figure 3 reveals an interesting pattern. Patients with mental health problems typically do not present with a single issue but present a cluster of diagnoses. We know from the Cass Review that many of the children turning up at NHS Gender Services often had eating disorders or traumatic experiences besides gender distress. Hence, gender dysphoria might be the primary diagnosis or not. In 2012, for 50 % of all gender dysphoria diagnoses (including primary, secondary, and tertiary ones), gender dysphoria was the main diagnosis. In 2023, this share shrank to 35 % suggesting that patient profiles are more complex. If the diagnostic overshadowing of trans prevails, more and more mental conditions are not accurately treated.
Trends in Transgender genital surgeries
Retrieving data about what some coin the “last step of medical transition” was somewhat more challenging. As with diagnoses, surgeries are also assigned a code. For English clinics, genital surgeries as a part of medical transition are given the ominous code “X15. Combined operations for sexual transformation” in the NHS Hospital Admitted Patient Care Activity Statistics. This code is then broken down into “X15.1 Combined operations for transformation from male to female”, “X15.2 Combined operations for transformation from female to male” and “X15.8 Other specified operations for sexual transformation”. Even after extensive research, it was not clear whether or not these refer to genital surgeries alone or whether other surgeries such as mastectomies are included. However, when looking at data from a Freedom of Information Request to the Scottish Government (Scottish data is only available from 2014-2023), there are vastly more mastectomies in Scotland than “X15.2 Combined operations for transformation from female to male” in England (which might include mastectomies). Hence including mastectomies into X15.2 seems unrealistic given that England is about 10 times the population of Scotland. It is still possible that X15.2 includes hysterectomies because phalloplasty often involves a preceding hysterectomy. With a remaining degree of uncertainty, operations under X.15 done on male patients (self-identified female) can be roughly summarized into vaginoplasty while for female patients, it means phalloplasty and possibly the removal of the uterus.

In general, the number of genital surgeries in England has roughly increased by a factor of 5 since 2000 (Figure 4). Especially pre- and post-pandemic, the surge is very strong. In Scotland, genital surgeries are performed less and less although it is unclear whether some activity might be shifted from Scottish clinics to English clinics. Wales and Northern Ireland do not have surgical services, so from 2014 onwards the sum of England and Scotland is the UK-wide number of genital surgeries. Note that the number of surgeries does not necessarily match the number of patients.

When we break it down by sex (Figure 5), we see that ‘male-to-female’ surgeries are much more widespread, there is a dramatic uptick in ‘female-to-male’ surgeries in recent years. This is deeply concerning since the complications are numerous and surgical outcomes are often very poor. Given the long waiting lists, this seems to be only the beginning unless more public attention is directed at these procedures.

Another reason why particularly the uptick in phalloplasties should ring alarm bells is that the average age of patients (Figure 6) undergoing this procedure is much lower than their male counterparts. In the last year of available data for NHS England, the average age of female patients was 23 while being almost 20 years below the mean for males. In Scotland, there also seems to be an age difference although less pronounced than in the English data.
With all this data, it should be kept in mind that when we look at genital surgeries, we only estimate the tip of the iceberg of gender medicine. A minority of trans-identified individuals undergo genital surgery. More might ‘only’ do what is euphemistically called ‘top surgery.’ Many more will take cross-sex hormones.
Ending on a positive note: Others do worse

If you care about the damage medical transition does, the situation sometimes might appear bleak. But it needs to be said that the UK still does a decent job of containing the impact, much better than other comparable countries. While the US and Canada are known to be the Wild West of gender medicine, another maybe unlikely candidate shows that medical transition in the UK might be less widespread than commonly thought. Gathering official data from Germany’s Federal Statistical Agency on transgender genital surgeries and normalizing the data to the population size of the UK (England respectively) and Germany, we see that genital surgeries in Germany are more common by a factor of almost 4 relative to the UK in 2023. While in the late 2000s, numbers were somewhat comparable, the increase in the UK since the 2010s is nothing compared to the explosion of interventions taking place in German gender clinics. Capacity constraints or an inert NHS not catching up to demand might be a reason. In this area of medicine, this is a good thing.
The only thing that comes to mind would be to compare objective outcome parameters of patients who have been granted medical transition to ones who were refused it for some random reason.
Great piece! Thank you for this work.
1. I'd like a TL:DR explanation of "diagnostic overshadowing”. I guess you mean that there are many cases where gender dysphoria is NOT the main diagnosis and actually these surgeries are being done to people whose primary diagnosis is that they have "mental health issues". I hope I have got that right.
2. I knew about how data on gender is flawed because people's gender identity is recorded, not their sex - in prisons and the NHS and elsewhere. That's bad enough. But I had not realised that "there has been a severe censoring of information by NHS England as unlike with other surgical procedures age and other patient characteristics are no longer published after 2015." I wonder why that change was made and if FoI requests would reveal the data. Certainly, ages of patients would seem to be important data.
3. Is there any relevant NHS data on de-transitioners, including surgeries to attempt to undo what has already been done?